Telehealth for the Treatment of Serious Mental Illness
Telehealth for the Treatment of Serious Mental Illness and
Substance Use Disorders
EVIDENCE-BASED RESOURCE GUIDE SERIES
Content of the Guide
This guide contains a foreword and five chapters. The chapters stand alone and do not need to be read in order. Each chapter is designed to be brief and accessible to healthcare providers, healthcare system administrators, community members, policy makers, and others working to meet the needs of people at risk for, experiencing, or recovering from SMI and/or SUD.
The goal of this guide is to review the literature on the effectiveness of telehealth modalities for the treatment of SMI and SUD, distill the research into recommendations for practice, and provide examples of how practitioners use these practices in their programs.
FOCUS OF THE GUIDE
SMI and SUD impact millions of Americans. Barriers to accessing care include access to appropriate services and providers, stigma associated with SMI or SUD, and competing priorities (e.g., employment and caregiving responsibilities).
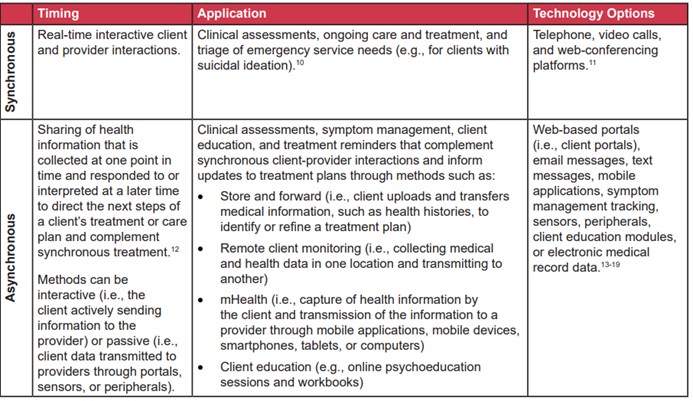
Telehealth is the use of two-way, interactive technology to provide health care and facilitate client provider interactions. Telehealth modalities for SMI or SUD may be synchronous (live or real time) or asynchronous (delayed communication between clients and providers).
Telehealth has the potential to address the treatment gap, making treatment services more accessible and convenient, improving health outcomes, and reducing health disparities.
Telehealth is the use of telecommunication technologies and electronic information to provide care and facilitate client-provider interactions. It is comprised of two forms:
1. Two-way, synchronous, interactive client provider communication through audio and video equipment (also referred to as telemedicine).
2. Asynchronous client-provider interactions using various forms of technology (further described in the chart below)
Serious mental illness (SMI) is defined as a mental, behavioral, or emotional disorder among adults aged 18 and older resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities.
Substance use disorder (SUD) is a diagnosis that applies when the recurrent use of alcohol or drugs causes clinically significant impairment, including health problems, disability, and failure to meet major responsibilities at work, school, or home.
Co-occurring disorder (COD) refers to the coexistence of both a substance use and mental disorder.
While telehealth is used in health care for a broad range of ages and presenting problems, this guide focuses on synchronous, direct to consumer (sometimes referred to as “D to C”) applications of telehealth for the treatment of SMI and SUD among adults.
Furthermore, this guide focuses on the needs of people experiencing SMI and SUD, but readers can broadly apply its resources and lessons for the treatment of any mental illness.
Background
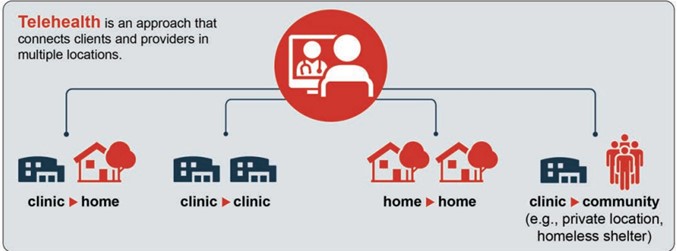
Telehealth can connect clients and providers in multiple locations such as at a home, private space in a clinical setting, or another location in the community. The graphic below depicts examples of ways to connect using telehealth, but there are many ways to deliver and receive care that address connectivity barriers and client preferences.
A variety of providers (e.g., psychiatrists, primary care providers, mental health counselors, social workers, psychologists, addiction counselors, case managers, opioid treatment providers, peer workers) can implement telehealth methods. In addition, practitioners can use telehealth with a hybrid approach or increased flexibility. For instance, a client can receive both in person and telehealth visits throughout their treatment process depending on their needs and preferences.
Telehealth methods can be implemented during public health emergencies (e.g., pandemics, infectious disease outbreaks, wildfires, flooding, tornadoes, hurricanes)21-25 to extend networks of providers (e.g., tapping into out-of-state providers to increase capacity).
They can also expand capacity to provide direct client care when in person, face-to-face interactions are not possible due to geographic barriers or a lack of providers or treatments in a given area.
However, implementation of telehealth methods should not be reserved for emergencies or to serve as a bridge between providers and rural or underserved areas.
Telehealth can be integrated into an organization’s standard practices, providing low-barrier pathways for clients and providers to connect to and assess treatment needs, create treatment plans, initiate treatment, and provide long-term continuity of care.
SMI and SUD impact millions of Americans.
However, for a variety of reasons and despite a perceived need, many do not seek treatment.
• Among adults aged 18 or older in 2019, 5.2 percent (13.1 million people) had an SMI. Of those, 47.7 percent (6.2 million people) reported an unmet need for mental health services in the past year.
• Among people aged 12 or older in 2019, 7.4 percent (20.4 million people) reported experiencing a SUD. Among people aged 12 or older in 2019, 7.8 percent (21.6 million people) needed substance use treatment in the past year. Of these 21.6 million people, 12.2 percent (2.6 million) received substance use treatment at a specialty facility.
Telehealth has the potential to address this treatment gap, making treatment services more accessible and convenient, improving health outcomes, and reducing health disparities.
Clients experiencing SMI and SUD have traditionally been excluded from both treatments delivered through telehealth and research evaluating the efficacy of telehealth among people experiencing SMI and SUD. However, telehealth is a tool that providers can use for all clients.
Appropriate and additional upfront work, provider client agreements, and safeguards can ensure that clients experiencing SMI and SUD benefit from services delivered via telehealth. Providers can use assessments (further discussed in Chapter 3) to identify their clients’ specific barriers to participating in telehealth appointments (e.g., access and comfort with technology, ability to have private or confidential conversations, safety of the home environment) and inform conversations with their clients on strategies to address these barriers.
Benefits of Telehealth
Telehealth supports team-based care and its interrelated care objectives. The Quadruple Aim is a conceptual framework to understand, measure, and optimize health system performance. The Quadruple Aim organizes benefits of telehealth into four categories:
• Improved provider experience
• Improved client experience
• Improved population health
• Decreased costs
1. Provider experience.
Providers may improve the quality of care they provide and experience the following benefits from implementing telehealth methods:
• Provision of timely client care. Providers may have increased flexibility in appointment scheduling by using telehealth. They can extend care beyond a clinic’s normal operating hours and its four walls and leverage “virtual walk-in visits.” Increased flexibility can help clinics to more effectively manage client “no-shows” and cancellations.
• Effective and efficient coordination of care. An estimated 40 to 60 percent of civilian clients (not inclusive of military populations) with mental and substance use disorders’ are currently treated in primary care offices rather than specialty
care settings.31 Providers can use telehealth methods for tele-consultation, tele-supervision, and tele-education to coordinate, integrate, and improve care (e.g., through the “hub and spoke” model).
• Reduction in workforce shortages. This is especially true for underserved and rural areas.
• Ability to assess client’s home environment.
Rather than rely on a client’s report of their home and living conditions, telehealth makes it possible for providers to see, with appropriate permission, inside a client’s home, meet family support systems, and determine if an in-person visit at a person’s home is needed.
READ MUCH MIRE INSIDE…
“TELEHEALTH FOR THE TREATMENT OF SERIOUS MENTAL ILLNESS AND
SUBSTANCE USR DISORDERS” $37

Click on the Blue Button Below for Instant Access!
Our 100% Money Back Guarantee:

If for any reason you decided within 30 days that “TELEHEALTH FOR THE TREATMENT OF SERIOUS MENTAL ILLNESS AND
SUBSTANCE USR DISORDERS” isn’t for you, simply notify us by email and we’ll gladly refund your money – no questions asked. That’s our Ironclad Guarantee!
The risk is entirely ours! You absolutely have nothing to lose!
Your name and email will Never be shared, sold, or given to anyone.
We keep our subscriber’s privacy sacred. We do not sell or rent your personal information to other parties. What’s more you can always unsubscribe at any time!
Warmest Regards, Coyalita
Behavioral Health Rehabilitative Specialist & Addiction Counselor
Copyright © 2021-2024 Thresholdlivecoyalita.com All Rights Reserved Privacy Policy – Earnings Disclaimer – Terms of Use – Contact Us




