Medicaid Handbook: Interface with Behavioral Health Services
Medicaid Handbook: Interface with Behavioral Health Services
Medicaid Handbook: Interface with Behavioral Health Services – Introduction Target Audience The target audience for this Medicaid handbook is composed of—
• State directors and administrators of mental or substance use disorder (M/SUD) services agencies
• Staff of state directors and administrators of M/SUD services agencies
• State network organizations for behavioral health services
• State Medicaid Authority staff involved with M/SUD services.
Generally, this handbook should prove useful to anyone wishing to learn the fundamental principles of Medicaid and apply them to their existing knowledge of behavioral health services.
Purpose
This handbook is intended to provide the reader with a basic understanding of the Medicaid program. There is a specific emphasis on the interplay between Medicaid principles and behavioral health services.
The goal is for the reader to navigate his or her state Medicaid program so that he or she can contribute meaningfully to policy conversations related to provision of behavioral health services to individuals who are eligible for Medicaid.
Throughout this document, the term behavioral health encompasses both mental and substance use disorders. When a mental or substance use disorder is addressed singularly, the reference will be only to that disorder.
Because each state’s Medicaid program is different from all others and because Medicaid laws and policies are ever changing, this handbook cannot contemplate every permutation of program construction. Rather, it is intended to provide enough structural framework and references to primary source documentation that someone wishing to gain a deeper understanding of his or her state’s program will have the necessary tools.
Module 1: Medicaid’s Importance to Mental Health and Substance Use Services
What is Medicaid’s Role in Behavioral Health Services?
Medicaid plays a significant role in the financing of treatment for mental or substance use disorders (M/SUDs). Together, services to treat mental and substance use conditions are referred to as behavioral health services. Although spending on behavioral health services is a small portion of all-health care spending (7.3 percent in 2005), it has a large impact on Medicaid spending. This is expected to increase under the Affordable Care Act’s A expansion of Medicaid coverage that is discussed more thoroughly in Module 7.
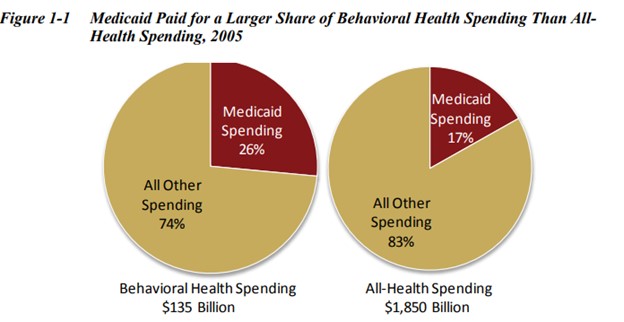
The Federal-State Medicaid program is currently the single largest funder of behavioral health services. B Nationally, Medicaid paid for 26 percent of behavioral health services, but only 17 percent of total all-health spending in 2005 (see Figure 1- ). “All-health spending” is the total spending on all behavioral health and physical health acute and long-term care services.
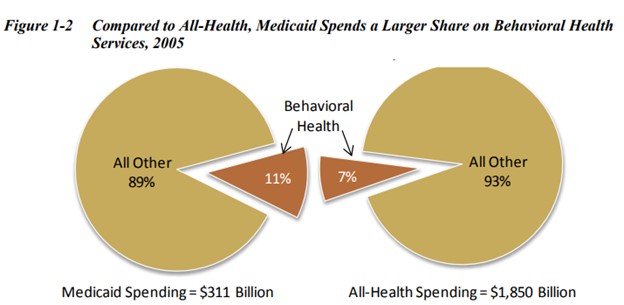
In addition to Medicaid paying for a large share of behavioral health services, behavioral health services account for a larger share of Medicaid benefits than it does of all health care services. Spending on behavioral health services accounted for 11 percent of Medicaid spending in 2005, but only 7 percent of spending by all-health care payers, as illustrated in Figure 1-2.
How Has Medicaid Spending on Behavioral Health Changed Over Time?
Medicaid spending on behavioral health treatment has increased from $6.6 billion in 1986 and to $35.7 billion in 2005. Along with the increase in spending, Medicaid’s share of funding for behavioral health services has risen—from 16 percent to 26 percent of behavioral health spending (see Figure 1-3).
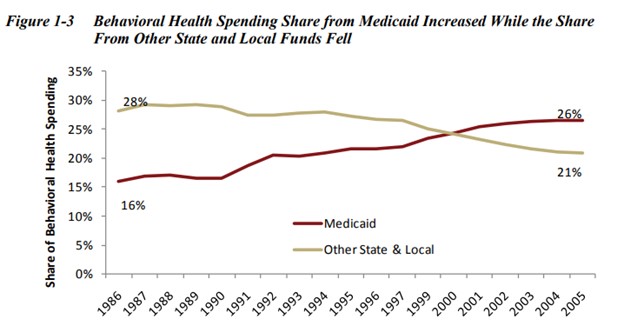
Although other non-Medicaid state and local spending on behavioral health treatment has also increased (from $11.5 billion in 1986 to $28.2 billion in 2005), it has not risen as rapidly as overall behavioral health spending. This has resulted in non-Medicaid state and local spending falling as a share of behavioral health spending from 28 percent in 1986 to 21 percent in 2005, as illustrated in Figure 1-3.
Because states vary greatly in services required by their populations, availability of behavioral health facilities and providers, and economic factors, the mechanisms states employ to leverage funding for behavioral health services also vary.
For example, there is variation in the types of treatment services for M/SUDs covered under the rehab option and other Medicaid State Plan services across states, as well as waiver services. These options are discussed as part of the behavioral health benefit package section in Module 3.
Historically, inpatient hospitalization in state hospitals was the main treatment option for many behavioral health conditions. Over time, state behavioral health agencies have moved aggressively to develop a robust array of community services and relationships to serve those with mental or substance use disorders.
Medicaid financing has been a key to this shift. In many cases, the increasing reliance on Medicaid has facilitated the expansion of many needed and evidenced-based behavioral health services.
For example, the number of Assertive Community Treatment (ACT) programs generally did not grow until states took steps to fund ACT through the Medicaid State Plan rehab option. Other behavioral health services that expanded under Medicaid include crisis intervention, case management, and partial hospitalization, as well as paying for medications.
Despite dramatic expansion of community-based services and supports aided by Medicaid funding, Medicaid still has limits. For example, although Medicaid can pay for treatment, medications, and some recovery support services, it cannot pay for housing and some residential treatment.
How Does Medicaid Spending on Behavioral Health Compare to Spending by Other Payers?
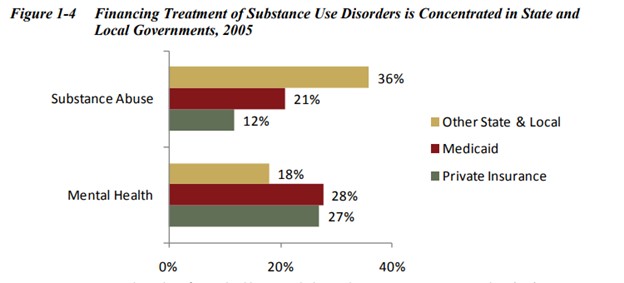
Services designed to treat SUDs are more likely to be financed by state and local governments, along with federal block grants, than by other payers, such as private insurance and Medicaid.
The total demand and aggregate costs are much higher for mental health services than for treating SUDs; however, state and local governments pay for a larger share of all substance use treatment services than mental health services, as shown in Figure 1-4.
The primary source of payments for similar behavioral health services may be quite different when comparing mental health services to treatment for SUDs. For instance, because of federal restrictions, residential treatment services for SUDs rely primarily on state and local government funding. On the other hand, Medicaid is the largest single financer of mental health residential support services. This sometimes reflects inclusion of different types of treatment professionals or variations in programmatic approaches that may be more or less “medical” in nature.
The disparity between private insurance coverage and Medicaid and other state and local funding is smaller for inpatient services, but much more substantial for residential treatment, as shown in Figure 1-5.
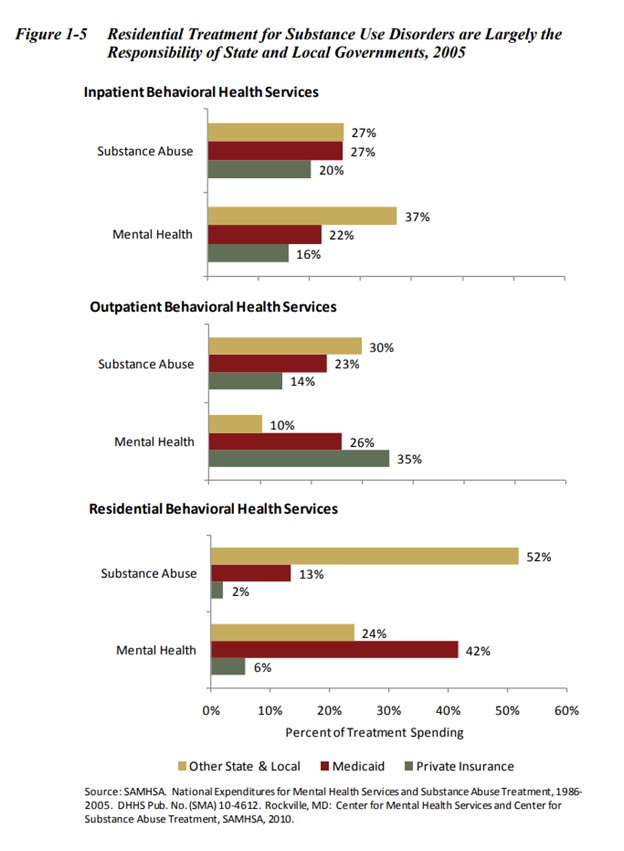
Historically, private health insurance has not covered inpatient hospitalization in state psychiatric hospitals, as well as some other services provided through the publicly funded behavioral health system. Thus, these publicly funded behavioral health services were primarily viewed as SafetyNet services. This has led to a disparity in funding from private health insurance for outpatient treatment of SUDs and of all residential services.
In addition to changes resulting from the Affordable Care Act, the Mental Health Parity and Addiction Equity Act (MHPAEA) of 2008 plays an important role in addressing this disparity, as discussed in Module 7.
READ MUCH MORE INSIDE.. 197 Pages
“MEDICAID HANDBOOK: INTERFACE WITH BEHAVIORAL HEALTH SERVICES” $39.40

Our 100% Money Back Guarantee:

If for any reason you decided within 30 days that “MEDICAID HANDBOOK: INTERFACE WITH BEHAVIORAL HEALTH SERVICES” isn’t for you, simply notify us by email and we’ll gladly refund your money – no questions asked. That’s our Ironclad Guarantee!
The risk is entirely ours! You absolutely have nothing to lose!
Your name and email will Never be shared, sold, or given to anyone.
We keep our subscriber’s privacy sacred. We do not sell or rent your personal information to other parties. What’s more you can always unsubscribe at any time!
Warmest Regards, Coyalita
Behavioral Health Rehabilitative Specialist & Addiction Counselor
Copyright © 2021-2024 Thresholdlivecoyalita.com All Rights Reserved Privacy Policy – Earnings Disclaimer – Terms of Use – Contact Us




