Rural Behavioral Health Telehealth
Rural Behavioral Health
Telehealth Challenges and Opportunities
This In Brief looks at common acceptability, availability, and accessibility barriers to mental and substance use disorder (behavioral health) treatment and services in rural*
* There are many definitions of rural, even within the federal government. This In Brief uses the word rural in a general sense to refer to areas of the United States that are sparsely populated communities and presents ways telehealth can help surmount some of these barriers.
Challenges to implementing effective telehealth services in sparsely populated areas are also discussed. This information is designed to be useful to behavioral health practitioners and many other professionals—such as attorneys, behavioral health training program faculty, clergy, pharmacists, and primary care practitioners—who are concerned with behavioral health in their communities. These professionals may be local centers of influence to whom others turn for behavioral health information and help. For more information on the use of telehealth for behavioral health service see shttp://store.samhsa.gov/product/TIP-60-Using-Technology-Based-Therapeutic-Tools-in-Behavioral-Health-Services/SMA15-4924
The term telehealth† “Telehealth is different from telemedicine because it refers to a broader scope of remote healthcare services than telemedicine. While telemedicine refers specifically to remote clinical services, telehealth can refer to remote non-clinical services, such as provider training, administrative meetings, and continuing medical education, in addition to clinical services.”18 refers to using internet and communications technologies (ICTs), such as video conferencing, chat, and text messaging, to provide health information and treatments in real time.
Telehealth also includes exchanging information and delivering services asynchronously, such as through secure email, webinars, or “store-and-forward” practices, which include videotaping a client encounter and forwarding the video to a professional who is offsite, for analysis at a later time.
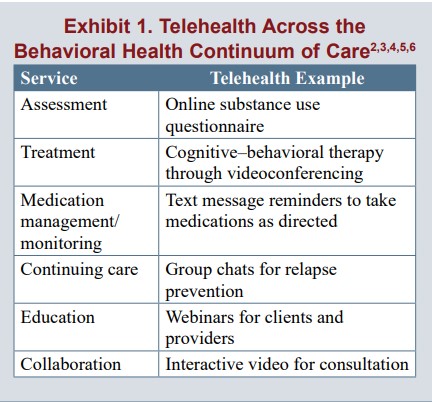
As access to at least some types of ICTs increases across the United States, the potential for telehealth also increases. Increasing levels of access create opportunities for providers to address rural–urban disparities across the behavioral health continuum of care (see Exhibit 1)
Nearly one in five U.S. residents lives in a rural area.7 According to most estimates, individuals living in rural locations experience mental and substance use disorders at rates that are similar to (and sometimes higher than) those of their urban counterparts.8,9,10,11,12,13
In a survey of rural health stakeholders, when participants were asked to identify the top 10 rural health priorities from a larger list of focus areas, they ranked mental health and mental disorders fourth and substance abuse fifth.
Despite having a similar need for services, people in rural areas have less access to the behavioral health continuum of care than do people in urban areas.15,16
Although funding cuts, workforce shortages, and other systemic issues hinder access to timely and appropriate behavioral health treatment and services in urban and rural areas alike, people in rural areas face additional barriers, such as a lack of adequate internet infrastructure,19,20 a need to travel long distances to see specialty providers, and a lack of anonymity about receiving treatment.
The idea of using telehealth to expand access to care first surfaced in the 1960s.22 Technology can facilitate the delivery of behavioral health services to people in rural areas in two main ways: (1) by linking clients to behavioral health practitioners located at a different site, and (2) by connecting nonspecialists in rural areas— commonly primary care practitioners—to networks of behavioral health specialists throughout the country for case consultation.
Acceptability Barriers
Treatment acceptability refers to whether patients consider treatment to be relevant, beneficial, and worthwhile. There is evidence that some rural communities normalize substance use and certain types of mental illness, such as depression, making it difficult for residents to judge when their condition warrants treatment.21,24,25,26
Numerous other factors influence whether individuals believe treatment is an acceptable response to their condition. For instance, a history of the U.S. agricultural population’s behavioral health care cites a culture of self-reliance as one reason this population tends to “avoid seeking behavioral healthcare even when needed.”27
Two major acceptability barriers facing individuals living in rural locations are a lack of privacy about receiving treatment for behavioral health conditions and a lack of culturally appropriate
care.
Lack of privacy
Individuals living in rural locations commonly identify a lack of privacy as a barrier to receiving treatment.15,28,29,30 Associated with the lack of privacy is the desire to avoid being the subject of gossip or being marginalized.21,30 In small communities, residents may recognize whose car is in a therapist’s parking lot, for instance.
Focus groups have revealed that certain cultural attitudes and beliefs may also contribute to a lack of privacy, exemplified by one study involving a faith community of rural African American individuals (see textbox at right).
Depression in a Rural African American Community
Focus groups with rural African Americans in a faith community revealed individual and cultural barriers to seeking treatment for depression.
Participants said that private information spreads easily through rumors in their small community, increasing the likelihood that individuals experiencing depression would be judged by others they see regularly.
Fear of being labeled “crazy” prevented people with depression from seeking care.
In addition, participants wanted to keep their “personal business” to themselves, and also did not want to pry into anyone else’s business. These attitudes sometimes kept them from knowing that friends needed help, as one participant discovered when he happened to visit a friend who had just taken pills in an attempt to take his own life.
Another barrier was the belief that depression is a normal part of everyone’s life. In a depressed environment, one participant said, individuals may not even recognize that they are depressed; the condition is viewed as a norm, not as an illness that requires treatment.
However, as in urban areas, factors besides race and ethnicity contribute to the formation of distinct cultures. In a rural area, these factors include the economic base (e.g., farming, forestry, manufacturing, tourism); proximity to urban centers; and any major subpopulations, such as seniors or veterans.
Medical and behavioral health researchers and practitioners working in rural areas have noted the dire need for behavioral health treatment and service practitioners who understand the needs of farmers and ranchers, veterans, and tribal communities and other ethnic and racial minorities.
READ MUCH MORE INSIDE…
DOWNLOAD YOUR COPY NOW ONLY $9.95

Click on the Blue Button Below for Instant Access!
Just use your name and valid email address – I will never sell or share your email address with anyone. Never. You may unsubscribe anytime. I hate spam just as much as you do.
Regards, Coyalita
Behavioral Health Rehabilitative Specialist & Addiction Counselor
Copyright © 2021-2024 Thresholdlivecoyalita.com All Rights Reserved Privacy Policy – Earnings Disclaimer – Terms of Use – Contact Us




